Electronic Health Records: a murderous, publicly subsidized, $13B/year grift by way of shitty software
In 2009, the bipartisan HITECH Act pledged $36 billion to subsidize the adoption of Electronic Health Records throughout America's fragmented, profit-driven health system, promising that the system would modernize American health care, save $80 billion (and countless lives), and deliver a host of other benefits; a decade later, the EHR industry has blossomed from $2B to $13B, and adoption is up from 9% to 96%, and it's a catastrophe.
Part of the problem lies in the structure of the HITECH Act itself: it created incentives for practices to buy "certification" EHR tools, but that certification was incredibly lax and allowed all kinds of terrible, buggy code to attain certification. The cash incentives were so great that companies poured fortunes into luring doctors to banquets where they were instructed on how to maximize their government subsidies, but the certification process did not protect doctors from unscrupulous vendors.
Importantly, a certified tool did not have to be standards-based, meaning that there was no requirement that patients be able to move their records from one practice to another (this is a feature, not a bug: the medical industry's term for a patient switching practices is "leakage," and the incompatibilities in rival practices' EHR tools were an excellent hedge against it, serving as a lock-in for patients). What's more, certified vendors were allowed to bind the healthcare providers to nondisclosure and nondisparagement clauses, making it illegal for them to warn other doctors about defects in EHR products.
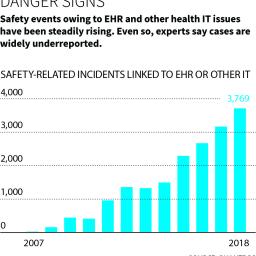
To top things off, the HITECH Act did not establish any kind of FDA tracking system for complaints about bugs in EHR tools -- even bugs that maimed or killed patients.
The result is a predictable litany of grifter software: badly written spaghetti code that deletes doctor's notes, fails to assign meds to matients, assigns meds to the wrong patients, fails to delete meds when discontinued, and can't even merge records -- a test of one vendor's software found that it failed to merge duplicate records correctly half of the time.
EHRs are the bane of American doctors. They throw a steady stream of false-positive warnings -- a doctor might see hundreds of these in a day, such as a warning that a 6-year-old girl (or boy!) should be checked for pregnancy before a medicine is given to them -- combined with crazy, overcomplexified, redundant UIs that require doctors to click the same thing in multiple places for it to stick. An ER doctor makes about 4,000 clicks in their EHR terminals in a single shift.
With such terrible, numbing repetition, it's no wonder that the industry refers to EHRs as "Errors Happen Regularly." The systems are incredibly dehumanizing for doctors, who spend six hours/day editing EHRs (44% of that work is clerical, not related to patient care), and is cited as a major contributor to the physician burnout crisis, which has led to mass exodus from medicine as well as a string of awful suicides.
But there are some advantages to EHRs for medical practices: they're practically designed to facilitate and disguise "upbilling" (a euphemism for insurance fraud).
Despite this confluence of interests between crooked practices and crooked EHR vendors, there have been many high-profile lawsuits and regulatory action (a $155m False Claims Act settlement with Eclinical works, another for $57m with Greenway Health).
And EHRs have done some good: they've been vital in unraveling the true story of the opioid epidemic, and were used to diagnose lead as the underlying cause of the Flint water crisis.
But it's a bad tradeoff: a $36B public subsidy, the needless death and injury of American patients, the dehumanizing and demoralizing of doctors, all to make some forensics work marginally simpler.
A well-designed EHR program would, at the very least, mandate standards-defined interoperability, a ban on nondisclosures and nondisparagements, full source-code publication, and public tracking and redress for bugs in EHR systems. Without those, the HITECH Act was born to fail.
"You're sitting in front of a patient, and there are so many things you have to do, and you only have so much time to do it in - seven to 11 minutes, probably - so when do you really listen?" asked John-Henry Pfifferling, a medical anthropologist who counsels physicians suffering from burnout. "If you go into medicine because you care about interacting, and then you're just a tool, it's dehumanizing," said Pfifferling, who has seen many physicians leave medicine over the shift to electronic records. "It's a disaster," he said.
Beyond complicating the physician-patient relationship, EHRs have in some ways made practicing medicine harder, said Dr. Hal Baker, a physician and the chief information officer at WellSpan, a Pennsylvania hospital system. "Physicians have to cognitively switch between focusing on the record and focusing on the patient," he said. He points out how unusual - and potentially dangerous - this is: "Texting while you're driving is not a good idea. And I have yet to see the CEO who, while running a board meeting, takes minutes, and certainly I've never heard of a judge who, during the trial, would also be the court stenographer. But in medicine"""we've asked the physician to move from writing in pen to [entering a computer] record, and it's a pretty complicated interface."
Even if docs may be at the keyboard during visits, they report having to spend hours more outside that time - at lunch, late at night - in order to finish notes and keep up with electronic paperwork (sending referrals, corresponding with patients, resolving coding issues). That's right. EHRs didn't take away paperwork; the systems just moved it online. And there's a lot of it: 44 percent of the roughly six hours a physician spends on the EHR each day is focused on clerical and administrative tasks, like billing and coding, according to a 2017 Annals of Family Medicine study.
For all that so-called pajama time - the average physician logs 1.4 hours per day on the EHR after work - they don't get a cent.
Where Electronic Health Records Went Wrong [Fred Schulte/Kaiser Health News; and Erika Fry/Fortune]
(via Naked Capitalism)